
Your Dental Office's Billing Model Is Backwards. Here's Where It Breaks.
Walk into almost any dental office and you'll find a revenue cycle operation (or dental billing, either inhouse or outsourced) built to clean up messes: front desk teams chasing insurance discrepancies, billers working aging reports, office managers auditing claims, outsourced billing companies fixing exceptions, and providers wondering why collections never seem to match production. It looks like a normal part of running a practice. It's actually compensation, an entire workflow designed to survive a problem nobody fixed at the source.
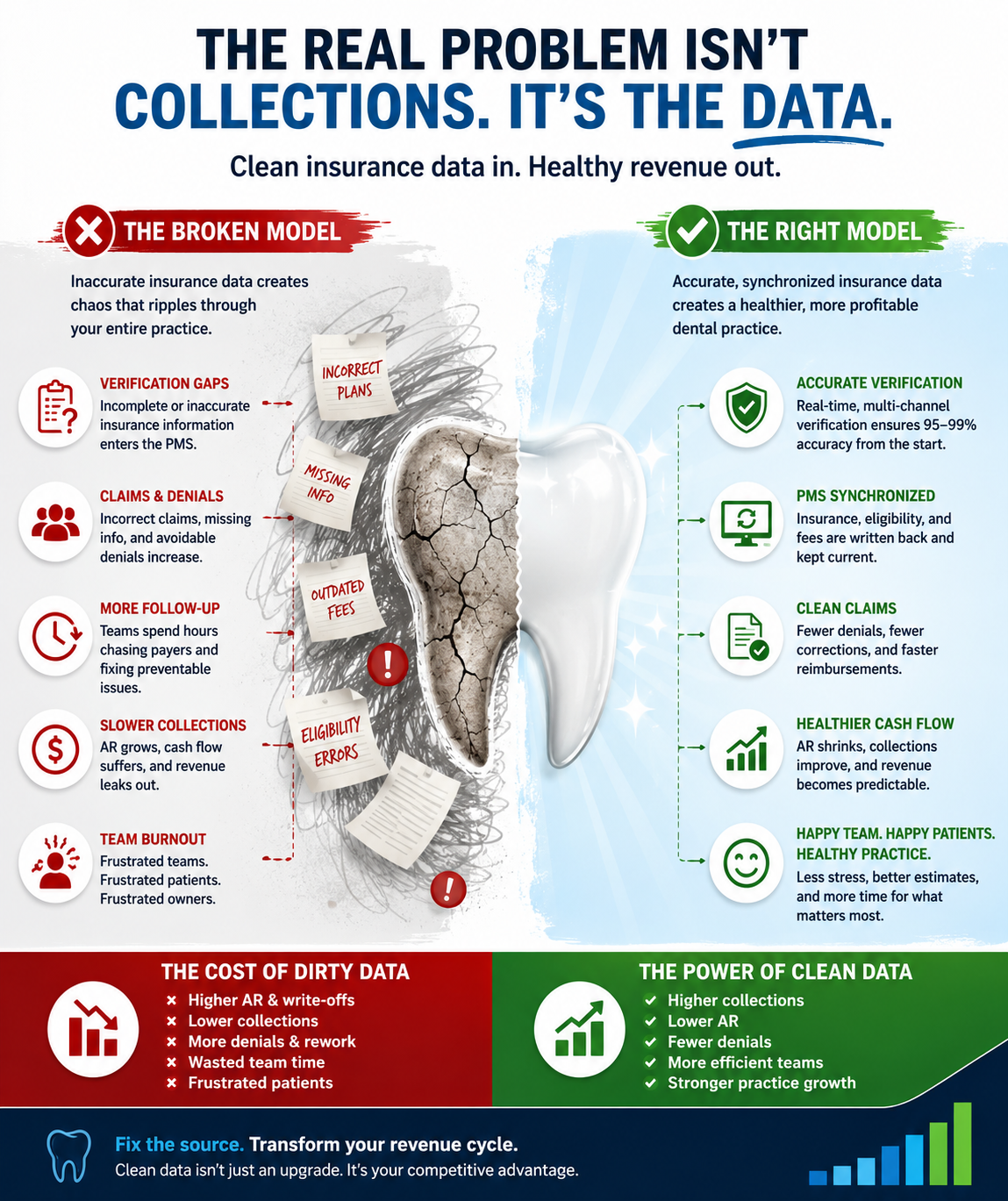
The problem is the insurance data entering the practice management system in the first place.
The industry quietly accepted, years ago, that insurance verification would always land somewhere around 70 to 85 percent accuracy. Front desks would patch the gaps. Team members would rush through eligibility checks between answering phones and checking patients in. Billers would catch the rest weeks later. We accepted that as the natural state of dentistry, and then built expensive processes around it.
It's worth asking whether the entire model is simply wrong.
The Hardest Problem in dental billing Isn't the One Everyone Talks About
Ask most dental office owners what the hardest part of revenue cycle management is and they'll say collections, payment posting, claim follow-up, or accounts receivable. Those are challenging. But they're challenging downstream. They're difficult because of what flows into them.
The genuinely difficult problem is achieving highly accurate insurance verification before the patient ever sits in the chair, and then keeping the practice management system continuously synchronized with the payer's source of truth as plans, fee schedules, frequencies, and eligibility change.
That last stretch of accuracy is where most organizations quietly give up. The jump from 85 percent to 95-plus percent means solving the ugly cases:
- Subleases and stacked plans
- Employer group mismatches
- Medicaid and managed care edge cases
- Coordination of benefits
- Outdated or incorrect fee schedules
- Years of legacy PMS contamination
- Incomplete portal data and conflicting phone-call answers
- Incorrect coverage tables and group plans
Most solutions stop short of this layer on purpose. It's operationally expensive, technically demanding, and requires years of payer-specific knowledge. So the gap remains, and around it, practices build workflows whose entire purpose is correcting errors that never needed to exist.
What Happens When You Actually Close the Gap
Run insurance verification consistently at 95 to 99 percent accuracy, with results written directly back into the PMS, and the rest of the revenue cycle begins to behave differently almost immediately.
Payment posting becomes easier because there is less to investigate. Claim reconciliation improves. Underpayments become easier to identify because you finally know what correct reimbursement should look like. Patient estimates become more accurate. Front desk stress decreases. Collections improve. Accounts receivable naturally declines because fewer claims are broken before they are submitted. Denials fall. Reporting becomes something you can actually trust.
The real shift is structural: the PMS stops being a liability and becomes a reliable financial system. That single change makes everything else look easier in hindsight.
Why We Keep Adding Labor Instead of Fixing the Source
When data is dirty, the rational short-term move always appears to be adding more labor.
Hire another biller.
Add another insurance coordinator.
Outsource billing.
Have the office manager review claims.
Bring in a consultant.
Add another layer of reporting.
Each solution relieves pain temporarily.
But none of them address the source of the problem. So costs continue to compound. Dirty PMS data quietly produces inaccurate treatment estimates, delayed collections, endless claim corrections, manual audits, frustrated patients, team burnout, and revenue leakage that rarely appears on a dashboard.
You don't pay for it in one obvious expense.
You pay for it in dozens of small inefficiencies that accumulate every single day.
This is operational debt.
And like any debt, it becomes more expensive the longer it remains unpaid.
The Future Belongs to the Cleanest Data, Not the Largest Team
For years, fixing insurance verification at the source wasn't realistic for independent dental practices. The labor required was simply too expensive.
That constraint is disappearing.
AI-driven verification, payer portal automation, omnichannel verification workflows, direct PMS writebacks, continuous synchronization, and exception-only workflows now make it possible to solve the problem where it actually begins.
The practices that adopt these technologies early won't win because they hired more people.
They'll win because they stopped needing to.
Clean data upstream allows front desk teams to focus on patient experience instead of insurance research. It gives billers fewer fires to put out. It allows office managers to manage growth rather than chase exceptions. Most importantly, it gives practice owners financial data they can actually trust when making decisions.
The future of dental operations won't belong to the practice with the biggest billing team.
It will belong to the practice with the cleanest data — and the confidence to build on top of it.